Circadian rhythm of the HPA axis and stress factors
In principle, the physiological circadian rhythm of the HPA axis is regulated at the level of the hypothalamus [7], specifically by the region of the suprachiasmatic nucleus (SCN), located immediately above the optic chiasm and connected to the retina through the retinohypothalamic tract. This region is linked to the paraventricular nucleus (PVN), the main site of CRH (Corticotropin Releasing Hormone) synthesis. CRH receptors in the adenohypophysis (anterior nucleus of the pituitary gland) control the synthesis and release of ACTH (AdrenoCorticoTropic Hormone or corticotropin) into the bloodstream. ACTH acts on the membrane receptors of corticoadrenal cells, stimulating the production of several hormones, predominantly cortisol (as well as other glucocorticoids, mineralocorticoids, dehydroepiandrosterone, and sex hormones) [HPA axis index - BIA-ACC].
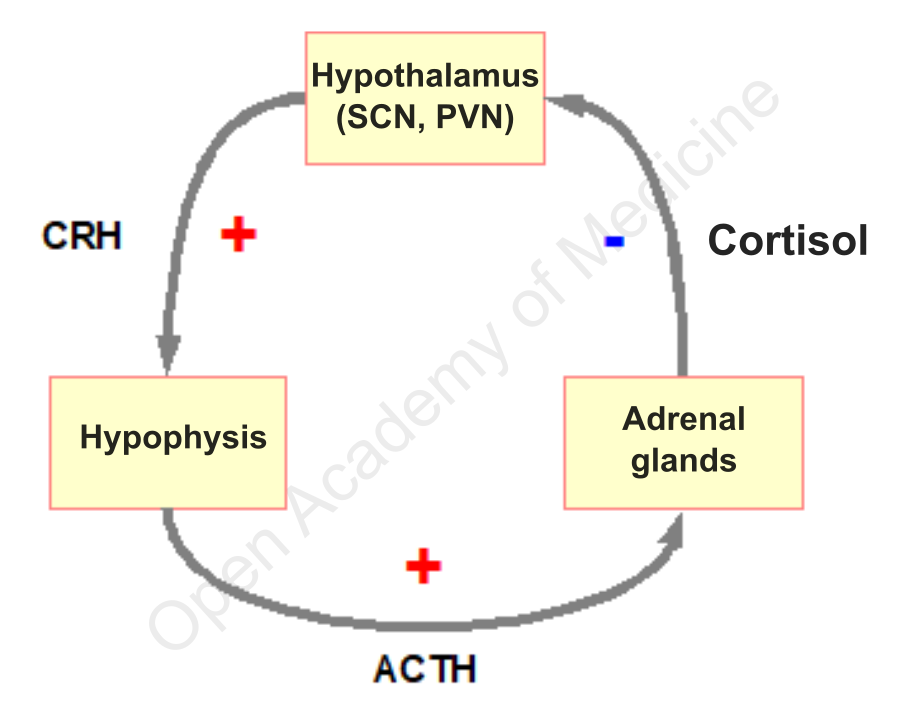
Figure 1: Diagram of HPA axis interactions
In the brain, mineralocorticoid receptors (MC) in the hippocampus bind cortisol with high affinity, while there is lower affinity for cortisol binding to glucocorticoid receptors (GC) in the hypothalamus, the hypophysis and in other areas of the brain structure. The type of receptors involved in cortisol binding is a factor which is directly involved in maintaining the circadian rhythm of CRH release: bindings to mineralocorticoid receptors prevail early in the night (during the phase of lower cortisol levels), whereas bindings to glucocorticoid receptors (in both the hypothalamus and hippocampus) are predominantly occupied in the acrophase of cortisol levels, thus increasing the inhibitory effect of cortisol on CRH and, consequently, ACTH secretion.
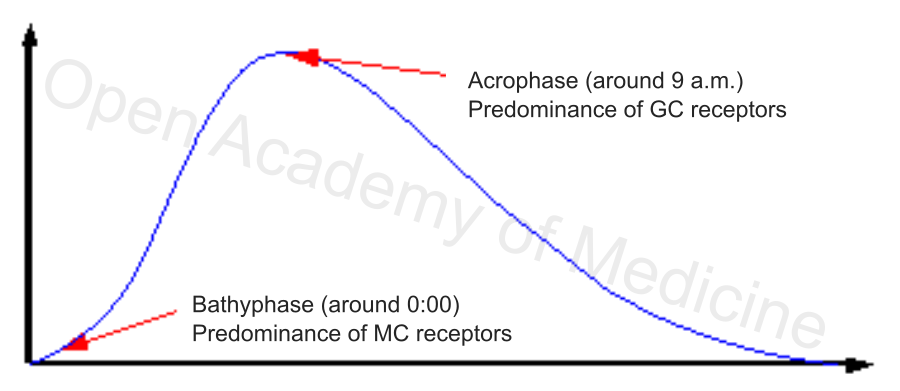
Figure 2: Physiological circadian rhythm of cortisol
One of the possible problems related to excessive cortisol concentration is the activation of glucocorticoid receptors in the amygdala [1,2,7] (causing a similar reaction to that due to excessive emotional stress), which occurs precisely when the level of cortisol is such as to have already somehow saturated hippocampus and hypothalamus receptors: this situation leads to a reversal of the physiological feedback of cortisol, stimulating the synthesis of CRH (proinflammatory at the peripheral level), with the extreme consequence of further stimulating the adrenal cortex to release cortisol – hence the loss of the physiological rhythm of the HPA axis as well as the modification of its homeostatic regulation.
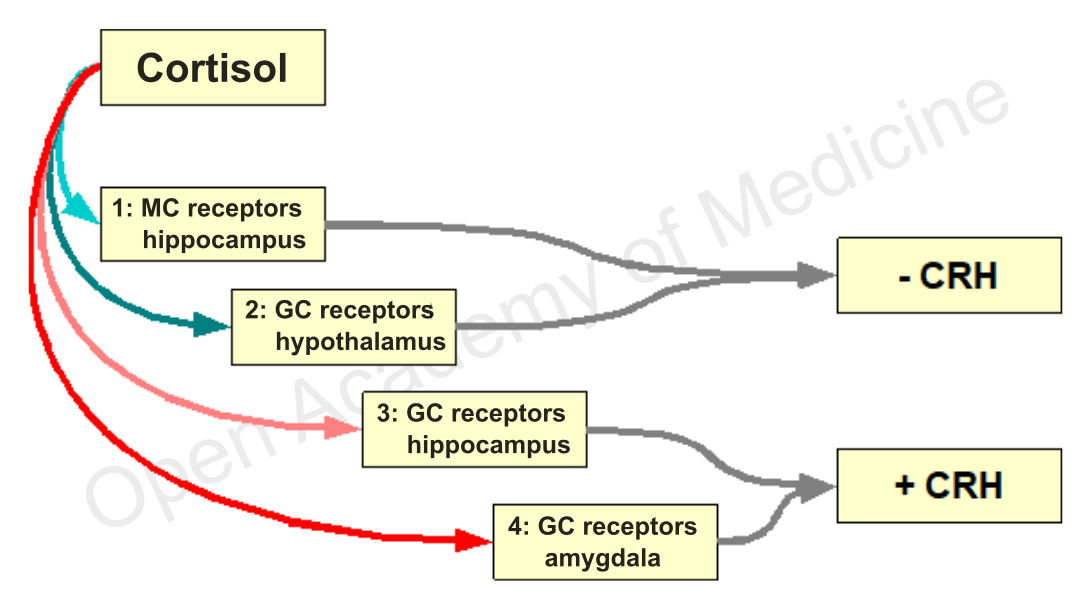
Figure 3: Cortisol bindings in the brain
Sleep disorders
Recent studies report that increased CRH secretion is associated with a decrease in the deepest sleep stage [6,7] and an increase in wakefulness. Electroencephalographic measurements have shown that, when CRH increases, δ (delta) frequencies [HF, LF, ANS-PPG Stress Flow], i.e., the lowest and most typical frequencies of the deepest sleep stages (called SWS, Slow-Wave Sleep), decrease.
The stressful activity due to the excess or loss of cortisol rhythmicity, which can easily correlate with chronic inflammatory states or poor nutrition [13] (see PPG Stress Flow, BIA-ACC and TomEEx diagnostic devices) – similarly to psychological or emotional stress factors involving strong reactions of the amygdala – thus leads to a drastic worsening of rest (and to the related chronic fatigue symptoms). This process represents a severe problem because the lower sleep quality increases in turn the activation of the HPA axis.
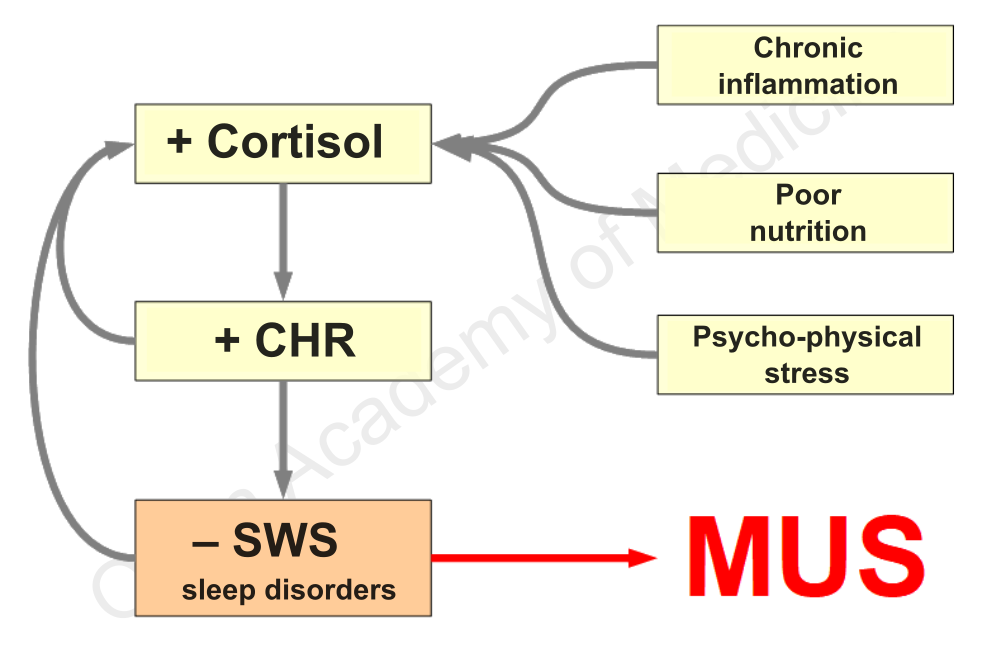
Figura 4: HPA, sleep disorders and MUS
Several sources have confirmed that chronic sleep deprivation is accompanied by elevated cortisol levels, particularly during the evening and the early night sleep. The evening cortisol level is also correlated with the number of nocturnal awakenings in both insomniacs and non-insomniacs.
A gradual recovery of the patient, aiming at lowering the evening cortisol level and restoring the circadian rhythm of the HPA axis through several methods (see RegMatEx and Biofeedback PPG Stress Flow devices), can therefore bring significant benefits, up to the disappearance of sleep-quality-related symptoms.
Mood disorders, MUS, anxiety, melancholy, depression, panic attacks
Many studies have emphasized the link between HPA axis dysfunction and several psychiatric syndromes [10,12], particularly evident in the case of depression. The stress reaction system basically consists in the release of CRH and noradrenaline (or norepinephrine), with the consequent stimulation of related systems, i.e. HPA axis [HPA axis index - BIA-ACC] and sympathetic nervous system [ANS - PPG Stress Flow] (increased heart rate, inhibition of insulin secretion, altered thermoregulation, etc.). The release of CRH (hypothalamus) and noradrenaline (locus coeruleus) in the brain are closely linked processes that can stimulate each other in order to prepare the body’s stress response. This involves, in addition to adrenal gland stimulation and the establishment of an unfavorable relationship between the secretion of cortisol and DHEA (dehydroepiandrosterone), the inhibition of insulin secretion. Interactions also closely involve the amygdala region [14,15], that acts as a mediator of emotional memory and of anxiety and fear behaviours.
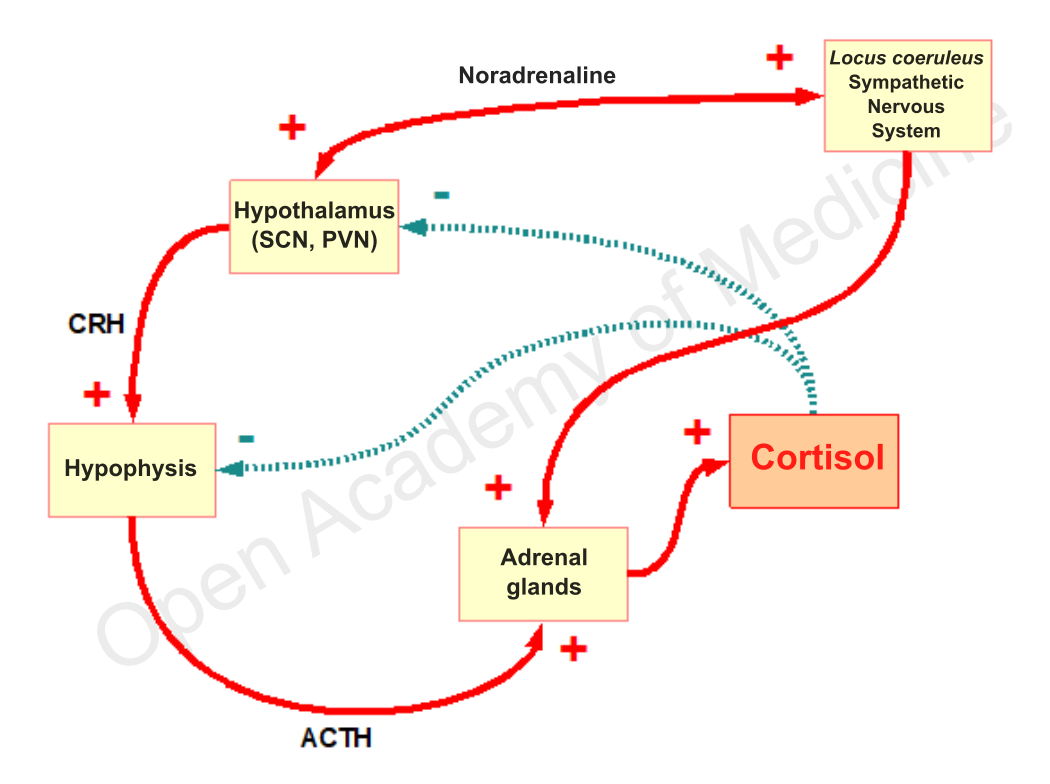
Figure 5: Hyperactivity of the HPA axis and sympathetic nervous system in anxious and depressive subjects
Many studies show the hyperactivity of the HPA axis [BIA-ACC - Flat Low/High HPA axis index], and the consequent neuroendocrine dysfunction, as a hallmark of anxiety-depressive disorders, to such an extent that it is considered a real method to distinguish between general melancholic states and clinical diseases [3,4,5]. The assessment of the impact of the stress level on the HPA axis (see TomEEx device in terms of functional impact, BIA-ACC device in terms of quantitative impact and PPG Stress Flow device in terms of impact in regulatory systems), the assessment of nutritional habits [13], and the gradual modulation of glucocorticoid levels (see RegMatEx device) remain therefore key aspects in the physiological approach to this type of disorders.
Authors: Dario Boschiero - Date: 04/11/2020
Attention: these contents can be freely used for personal learning purposes only. The use is regulated by Law No. 633/1941 and subsequent amendments, as well as by the copyright and patent legislation in force. Any use for commercial and profit-making purposes is forbidden.
References




