High-protein diets, low consumption of
negative-PRAL foods, excessive exercise, increased BMI and waist circumference,
elevated levels of glucocorticoids due to excessive stress and persistent activation of the stress system (
HPA - Axis index/ BIA-ACC, Biotekna), superficial breathing and/or altered respiratory rhythm and excessive intake of high-NaCl (kitchen salt) foods, such as for example white bread and its by-products, cold cuts, salami and seasoned cheese: all of these play a role in changing and straining the natural ability of kidneys and lungs to adapt to continuous pH changes. In point of fact, it is indispensable for our health to maintain proper pH levels [1].
Several authors in scientific literature have demonstrated long ago a close correlation between the increase in urine acidity (as a result of one or more of the above factors) and the risk of developing nephrolithiasis (i.e., the possibility to develop calcium oxalate or uric acid stones). Not only that, though. Indeed, what many do not know, is that impairment of the kidney function starts in healthy subjects with a high level fat (FM -
BIA-ACC, Biotekna). [2-4]
As a matter of fact, the reduction in urinary pH is one of the main defense methods used by our body to excrete the net acid load (a.k.a. NAE - Net Acid Excretion). Indeed, the kidneys’ ability to spend protons declines [5,6] subsequent to a disease, a diet that is too high in
positive PRAL foods, excessive exercise or high BMI.
![]()
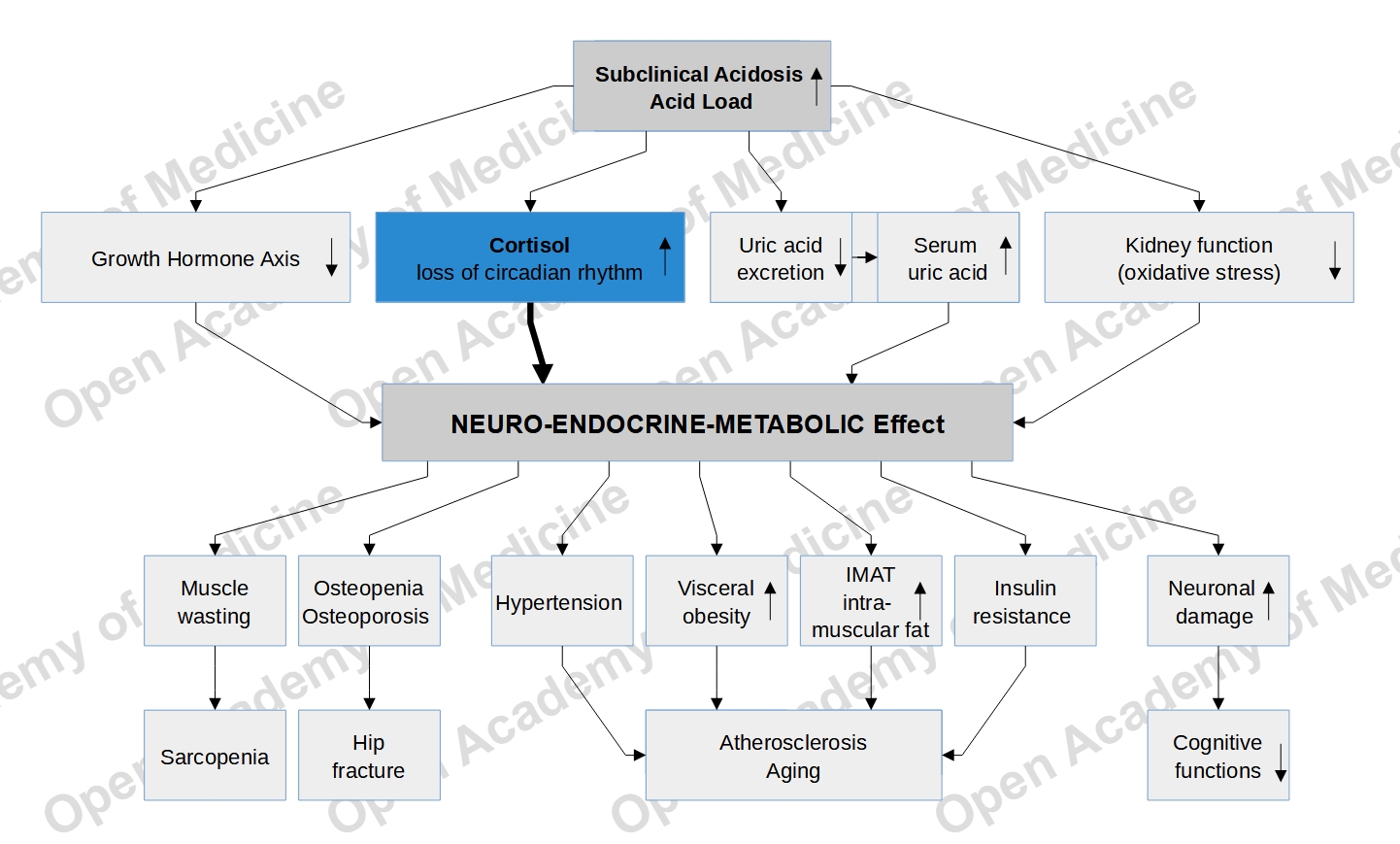
In the long run, high-positive-PRAL diets affect the blood acid/base characteristics - albeit less so in normal-weight patients, whereas in those with diseases or who are overweight the impact is more significant and long-lasting. For this reason, many diseases benefit from a diet that is high in vegetables, low in NaCl (kitchen salt) and supplemented (where needed) with buffer systems (with the single most important buffer system of the body being sodium bicarbonate). Examples include: gout, arterial hypertension, metabolic syndrome, insulin-resistance, osteoporosis, calcium oxalate stones, uric acid stones and hypocitraturia. [7,8]
Therefore, it is important to correct one’s diet by increasing
negative-PRAL foods, ensuring a water intake equal to approximately 4% of total body weight, reducing adipose tissue and
adding supplements that contain buffer systems, especially when, given the many variables that lead to a shift in the blood acid/base characteristics, a change to an improved net acid load can be to slow. (For example, in healthy subjects, this can be due to excessive exercise with poor recovery or shifting of the entire calorie load in the evening). [9,10]
Our body has counter-regulation processes (regulated by
vitamin D and by increased bowel reabsorption) that protect us from a sudden increase in calcium excretion. Still, this counter-regulation lacks magnesium. It is therefore useful to take
buffer supplements that contain, besides sodium carbonate, also magnesium and calcium, as the latter two provide support in case of increased calcium and magnesium excretion (which typically occurs with increased net acid excretion, i.e.
high NAE).
Benefits can be found by taking
buffer supplements with sodium carbonate, magnesium and calcium on an empty stomach (e.g.: 3 pills before breakfast, or before lunch or before dinner), with each pill accounting for approximately 10% of the RDA (recommended daily amount). In sports, these supplements are an excellent solution if taken before training as a buffer storage and after training to curb the effects of the temporary and natural production of post-exercise acidosis (3 pills before and/or after training).
Authors: Dario Boschiero, Mariantonietta Lucafò - Data: 27/11/2019
Attention: these contents can be freely used for personal learning purposes only. The use is regulated by Law No. 633/1941 and subsequent amendments, as well as by the copyright and patent legislation in force. Any use for commercial and profit-making purposes is forbidden.
References
- Leal VO, Delgado AG, Leite M Jr, Mitch WE, Mafra D. Influence of renal function and diet on acid-base status in chronic kidney disease patients. J Ren Nutr. 19(2):178-82; 2009
- Cameron MA, Maalouf NM, Adams-Huet B, Moe OW, Sakhaee K. Urine composition in type 2 diabetes: predisposition to uric acid nephrolithiasis. J Am Soc Nephrol. 17(5):1422-8. Epub 2006
- Trinchieri A, Zanetti G, Curr. A, Lizzano R. Effect of potential renal acid load of foods on calcium metabolism of renal calcium stone formers. Eur Urol. 39 Suppl 2:33-6; 2001
- Berkemeyer S, Remer T. Anthropometrics provide a better estimate of urinary organic acid anion excretion thana dietary mineral intake-based estimate in children, adolescents, and young adults. J Nutr. May;136(5):1203-8. 2006
- Remer T, Manz F. Potential renal acid load of foods and its influence on urine pH. J Am Diet Assoc. 95(7):791-7.1995
- Welch AA, Mulligan A, Bingham SA, Khaw KT. Urine pH is an indicator of dietary acid-base load, fruit and vegetables and meat intakes: results from the European Prospective Investigation into Cancer and Nutrition (EPIC)-Norfolk populationstudy. Br J Nutr. 2008 Jun;99(6):1335-43. Epub 2007
- Esche J, Krupp D, Mensink GBM, Remer T. Dietary Potential Renal Acid Load Is Positively Associated with Serum Uric Acid and Odds of Hyperuricemia in the German Adult Population. J Nutr. 148(1):49-55. 2018
- GBD 2017 Diet Collaborators. Health effects of dietary risks in 195 countries, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2019 May 11;393(10184):1958-1972. doi: 10.1016/S0140-6736(19)30041-8. Epub 2019
- Akter S, et al. High dietary acid load is associated with increased prevalence of hypertension: the Furukawa Nutrition and Health Study. Nutrition. 2015
- Malmir H, Saneei P, Larijani B, Esmaillzadeh A. Adherence to Mediterranean diet in relation to bone mineral density and risk of fracture: a systematic review and meta-analysis of observational studies. Eur J Nutr. 2018 Sep;57(6):2147-2160. doi: 10.1007/s00394-017-1490-3. Epub 2017